The History of Hyperbaric Oxygen Medicine
Table of Contents
1. The International History of Hyperbaric Oxygen Medicine
1.1 The Emergence of Hyperbaric Medicine
The emergence of hyperbaric medicine is closely linked to innovations in human diving activities and advances in our understanding of the physical laws governing gases under high pressure and the physiological changes in the human body. The origins of hyperbaric medicine can be traced back to ancient human diving activities. As early as 4500 BCE, there were already recorded instances of diving. At that time, due to the lack of specialized diving equipment, each dive could only last a few minutes, and the maximum depth was limited to within 30 meters. According to legend, Alexander the Great was the first person to use diving equipment to expand the limits of underwater activity. In 332 BC, during his conquest of Tyre (modern-day Sur, Lebanon), Alexander the Great placed himself inside a massive glass barrel to cross the Bosporus Strait and secure victory in the war (Figure 1-1-2-1). Beginning in the 16th century, various creative ideas and projects aimed at improving diving equipment flourished. Around 1500 AD, Leonardo da Vinci drew sketches of various diving devices, but did not develop any practical equipment. In 1620, the Dutch inventor Cornelius Drebbel developed the first true diving bell, which became the prototype for modern submarines. In 1691, Edmond Halley improved upon the diving bell technology by using high-pressure air from weighted barrels sunk to the seafloor to facilitate breathing. Over the next two centuries, high-pressure diving helmets and diving suits were developed, making it possible for people to remain underwater for an hour or longer.

Figure 1-1-2-1. Alexander crossed the Bosporus Strait in a glass barrel
With the widespread adoption of diving and improvements in diving equipment, medical issues related to high pressure began to receive attention; for example, increased water pressure can cause the eardrum to rupture. At the same time, those who ventured into deeper diving bells soon became aware of the most well-known medical problem associated with diving—decompression sickness. In the mid-19th century, it was discovered that re-exposing divers suffering from decompression sickness to high-pressure air could effectively alleviate their symptoms. From that point on, human understanding of hyperbaric medicine was no longer limited to adapting diving equipment to high-pressure environments and recognizing physiological changes in the human body under such conditions; it began to enter a phase of exploring the use of high pressure to treat diseases.
1.2 The Development of Hyperbaric Medicine
As one of the early medical technologies still in use today, the history of hyperbaric medicine dates back more than 350 years.
British physician Henshaw was the first doctor to attempt treatment using changes in air pressure. In 1622, Henshaw invented a hyperbaric chamber connected to a large organ bellows; by operating a series of valves and the bellows, he could make the air inside the chamber more concentrated (compressed) or less dense (decompressed), thereby treating certain acute or chronic diseases. Some of the patients treated by Henshaw experienced temporary improvement in their symptoms. Henshaw believed that “even for healthy individuals, the hyperbaric chamber is an effective method for aiding digestion, promoting respiration, and facilitating the expulsion of phlegm. Therefore, it is also highly effective in preventing most lung diseases.” However, since effective gas exchange could not occur within the chamber, the “encouraging” changes in respiration and other functions described by Henshaw may have been the result of the accumulation of metabolic waste products.
In 1832, French internist Émile Tabari conducted a series of studies to investigate the effects of reduced atmospheric pressure on the human body. Tabari claimed to have successfully treated 49 patients with respiratory diseases and believed that, due to its “indispensable nature,” the atmosphere, when properly regulated, would “provide an inexhaustible wealth of benefits to humanity.” Tabari’s most significant contribution to hyperbaric medicine was laying the foundation for today’s mainstream hyperbaric oxygen therapy protocols. He advocated for a gradual increase in atmospheric pressure, maintaining it steadily at a predetermined maximum—typically twice atmospheric pressure—and then slowly reducing the pressure, with the entire process taking approximately two hours.
In 1834, French physician Junod constructed the first hyperbaric chamber—a spherical chamber made of copper capable of being pressurized to 4.0 ATA. From then on, the process of continuously improving hyperbaric treatment equipment began. Three years later, Pravaud installed the largest cluster of hyperbaric chambers of that era in Lyon, France—capable of accommodating 12 patients simultaneously—and used hyperbaric air therapy to treat a variety of diseases, primarily lung diseases. Starting in the 1850s, hyperbaric air therapy became popular across much of Western Europe; countries such as the United Kingdom, Germany, the Netherlands, Belgium, and Austria successively established hyperbaric chambers. In 1860, hyperbaric chambers also began to appear on the North American continent. In addition to innovations in hardware, the scope of hyperbaric air therapy was constantly being explored; whenever a new disease was discovered, many researchers sought to treat it using hyperbaric air therapy. In 1855, Bertin authored the first textbook describing hyperbaric medicine.
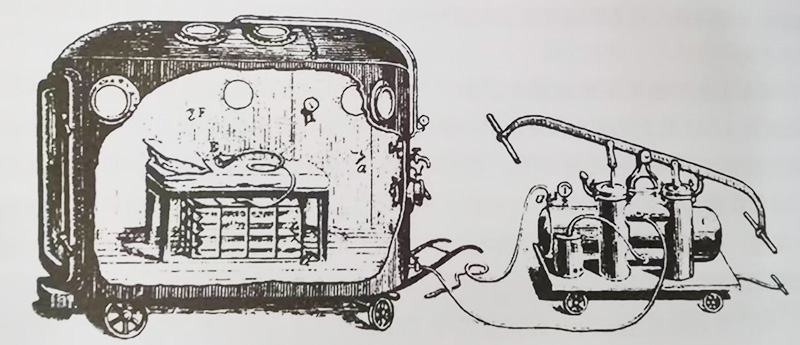
In 1877, Fontaine introduced a mobile hyperbaric operating room capable of accommodating 12 people (Figure 1-1-2-2), marking the first application of hyperbaric medicine in surgical procedures. Surgeons performed approximately 27 different types of surgeries in this hyperbaric operating room. All surgeries in the hyperbaric operating room were completed successfully. It was reported that, compared to conventional operating rooms, patients in the hyperbaric operating room required less time to recover from anesthesia, experienced milder vomiting symptoms, and did not exhibit cyanosis during surgery.
In the late 1880s, American neurologist Conning observed a large number of cases of paralytic decompression sickness while visiting the Hudson River Tunnel construction site and concluded that this condition was essentially an infection of the spinal cord. Cunningham discovered that hyperbaric oxygen therapy could significantly improve the neurological symptoms of such patients, so he extended its use to brain and spinal cord disorders unrelated to decompression sickness. Unlike his predecessors, Cunningham no longer regarded hyperbaric oxygen therapy as a standalone treatment but rather as an adjunct to drug therapy for neurological and psychiatric disorders—an approach similar to the current model of combining hyperbaric oxygen therapy with multidisciplinary treatment for various diseases.
Beginning in 1918, American anesthesiologist Cunningham used hyperbaric chambers to treat critically ill influenza patients and discovered that hyperbaric air therapy could restore consciousness and reduce cyanosis in some of these patients on the brink of death. These findings greatly inspired Cunningham. Over the next decade or so, Cunningham used hyperbaric oxygen therapy to treat a large number of patients suffering from influenza, lung diseases, arthritis, glaucoma, pernicious anemia, diabetes, syphilis, and certain cancers. He also conducted a series of theoretical studies related to modern hyperbaric medicine, such as discovering that oxygen levels vary across different tissues in the body, with oxygen tension being significantly lower in bones and connective tissues. In 1928, Cunningham constructed a massive, five-story-tall hyperbaric chamber to accommodate more patients for hyperbaric therapy. This move attracted the attention of the American medical community, and that same year, the American Medical Association requested that Cunningham provide relevant clinical data for peer review. Cunningham outlined the basis of his treatment but failed to provide supporting data. Consequently, he faced skepticism and criticism from the American medical community. Cunningham subsequently ceased his practice of using high-pressure air to treat diseases, marking the end of the era of high-pressure air therapy for therapeutic purposes—except for the treatment of decompression sickness.
1.3 The Rapid Development of Hyperbaric Oxygen Medicine
Due to the limitations of high-pressure air therapy and the discovery of oxygen, hyperbaric oxygen medicine gradually became the primary focus of research in hyperbaric medicine, and researchers began to continuously explore the range of diseases that hyperbaric oxygen might treat.
(1) Early Hyperbaric Oxygen Therapy The first practical application of hyperbaric oxygen therapy is attributed to a South American physician, though his contributions remain largely overlooked to this day. In 1934, Brazilian physician De Almeida reported central nervous system toxicity caused by hyperbaric oxygen, one of the earliest documented cases of hyperbaric oxygen therapy. De Almeida used 3.0 ATA hyperbaric oxygen in combination with radium to treat malignant tumors and discovered a synergistic effect between the two. Subsequently, de Almeida also studied the effects of hyperbaric oxygen on leprosy and chemical warfare agents, publishing his observations in multiple languages across various countries. Regrettably, his pioneering applications of hyperbaric oxygen did not attract widespread attention.
(2) Diving Medicine Shortly after de Almeida’s work, the U.S. Navy began using hyperbaric oxygen to treat decompression sickness. Their use of hyperbaric oxygen can be divided into two parts: the decompression process during which divers ascend from underwater to the surface, and the subsequent treatment in a hyperbaric oxygen chamber. Initially, divers who had been breathing air underwater had to significantly extend their decompression time upon returning to the surface to ensure safety; this process could last as long as 24 hours or more, which greatly affected the effectiveness of decompression sickness treatment. The U.S. Navy gradually began experimenting with nitrogen-oxygen mixtures in varying proportions as a substitute for air. Their research revealed that hyperbaric oxygen could accelerate the decompression process during a diver’s ascent to the surface and enhance the safety of this process. Consequently, during the decompression process upon returning to the surface, divers shifted from breathing air to breathing mixtures containing varying concentrations of oxygen and inert gases, or to breathing oxygen at a specific pressure.
In the 1960s, recreational diving began to gain popularity. Due to a relative lack of medical equipment compared to the Navy, treatment for decompression sickness patients in recreational diving was often delayed, and the effectiveness of traditional hyperbaric air therapy for decompression sickness was significantly reduced. After a series of studies, the U.S. Navy ultimately adopted hyperbaric oxygen therapy—involving the inhalation of oxygen inside a chamber—to treat decompression sickness, a practice that continues to this day.
(3) Radiation Sensitization: In the early 1950s, Gary and his colleagues observed that when laboratory mice were exposed to hyperbaric oxygen, the sensitivity of tumor cells in their bodies to radiation increased. These experiments laid the foundation for the use of hyperbaric oxygen as a radiation sensitizer. Gary’s team further observed that the radiobiological damage to tumor cells during radiation therapy depended on the oxygen concentration surrounding the tumor. In fact, many solid tumor cells exhibit varying degrees of hypoxia. These findings were sufficient to encourage researchers to conduct early clinical trials. A team at St. Thomas’ Hospital in London, England, conducted a series of clinical studies and found that even within the same patient, tumor regions treated with both hyperbaric oxygen and radiation exhibited more pronounced radiation damage than those treated with radiation alone.
More than a decade after hyperbaric oxygen was first used for radiation sensitization, doubts began to arise regarding its safety. Some studies suggested that patients who underwent hyperbaric oxygen-enhanced radiation therapy appeared to have higher rates of tumor recurrence and metastasis. At the same time, due to the lack of a clear and sustained survival benefit from hyperbaric oxygen therapy and the introduction of alternative radiation sensitizers, interest in hyperbaric oxygen-enhanced radiation therapy gradually waned and had essentially ceased by the mid-1970s.
1.4 Cardiac Surgery
Another significant hyperbaric oxygen event in the 1950s was the performance of cardiac surgery inside a hyperbaric oxygen chamber by Dutch cardiovascular surgeon Ita Burma, known as the “father of hyperbaric oxygen therapy.” Initially, Burma introduced controlled hypothermia, which doubled the tolerable ischemia time for cardiac surgery. However, even with this doubling, the total tolerable ischemia time for cardiac surgery was only about 5 minutes. At this point, Burma began to consider hyperbaric oxygen therapy. He lowered the body temperature of pigs and exposed them to 3.0 ATA oxygen, using a Ringer’s solution-like plasma substitute containing dextran. In his laboratory, although the animals’ hemoglobin levels dropped to virtually zero, there was still sufficient oxygen to support organ function and the survival of the animals. Burma published this research in the first issue of the *Journal of Cardiovascular Surgery* under the title “Life Without Blood.”
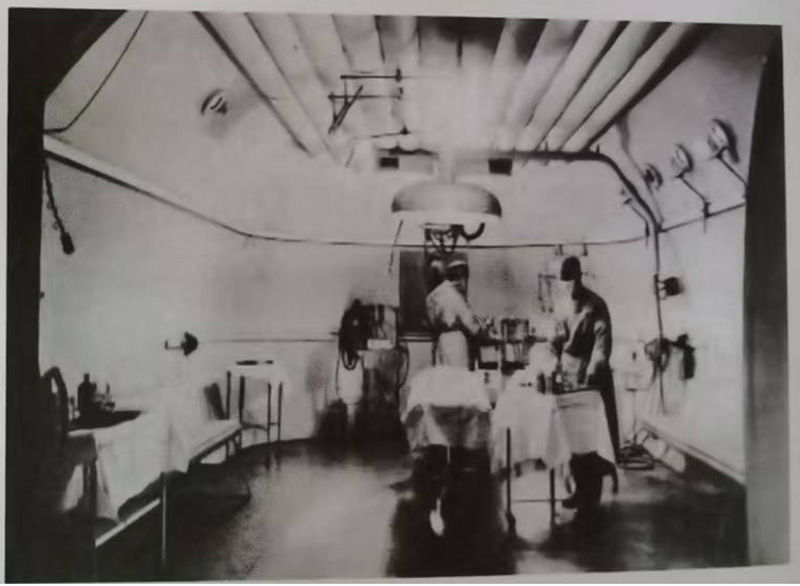
By 1959, Burma and his colleagues had constructed specialized hyperbaric operating rooms for performing cardiac surgery on infants and adults (Fig. 1-1-2-3, Fig. 1-1-2-4), thereby securing a sufficiently long tolerable ischemic time for cardiac surgery. Soon, many hospitals around the world were equipped with hyperbaric operating rooms. In 1963, Bernhard and his colleagues at Harvard Medical School developed several complementary technologies based on hyperbaric oxygen and hypothermia, one of which was a miniature extracorporeal circulation oxygenator, further ensuring the safety of cardiac surgery. At this time, cardiac surgery in hyperbaric chambers was in high demand. The development of extracorporeal circulation devices was also progressing steadily. As extracorporeal circulation technology gradually matured, the practice of cardiac surgery in hyperbaric oxygen chambers began to face difficulties, and hyperbaric oxygen gradually faded from the history of cardiac surgery. However, Burma’s proven theory—that hyperbaric oxygen can deliver sufficient oxygen to tissues and organs without relying on hemoglobin—ultimately became the foundation for the treatment of acute carbon monoxide poisoning, crush injuries, and other conditions involving acute ischemia and perfusion defects, as well as specific forms of hemorrhagic anemia.

1.5 Antimicrobial Effects
Shortly after introducing cardiac surgery in hyperbaric chambers, Burma treated a patient with gas gangrene—considered “incurable”—using hyperbaric oxygen therapy at 3.0 ATA. He observed that the previously progressive infection was dramatically halted, and the patient’s systemic toxic symptoms quickly subsided. Although oxygen was also injected directly into the tissues of soldiers with gas gangrene during World War I, the efficacy of hyperbaric oxygen therapy was significantly superior to that of traditional oxygen injection. Subsequently, an increasing number of animal and clinical studies were conducted. In a canine model of gas gangrene, researchers found that the best therapeutic outcomes were achieved when antibiotics, surgery, and hyperbaric oxygen therapy were used in combination. Numerous animal experiments and clinical data indicate that the distinct effects of hyperbaric oxygen therapy compared to conventional oxygen therapy are related to its ability to regulate oxygen free radicals, facilitate the transport of antibiotics across bacterial cell walls, and enhance leukocyte-mediated killing of aerobic microorganisms. Currently, hyperbaric oxygen therapy has been expanded to treat necrotizing soft tissue infections caused by aerobic, anaerobic, and mixed bacterial flora.
1.6 Wound Healing
In 1965, Japanese scientist Wada and his colleagues reported a case of a survivor of carbon monoxide poisoning from a coal mine fire who received hyperbaric oxygen therapy. They found that, compared to burn patients with carbon monoxide poisoning who did not require hyperbaric oxygen therapy, those who received the treatment exhibited better healing of their burn wounds. This observation prompted some researchers to investigate the therapeutic potential of hyperbaric oxygen therapy for burns; they discovered that it can reduce edema at burn sites, shorten healing time, lower infection rates, accelerate the restoration of capillary blood flow, and alleviate inflammatory responses. By the 1970s, hyperbaric oxygen therapy had gradually begun to be applied to the treatment of chronic wounds. The use of transcutaneous oxygen pressure measurements has aided in patient selection, identified non-responders, and provided recommendations for treatment endpoints. This screening process has improved the clinical outcomes and cost-effectiveness of hyperbaric oxygen therapy. Currently, the application of hyperbaric oxygen therapy for problematic wounds has expanded to include patients with arterial insufficiency, diabetes, and soft tissue radiation necrosis.
2. History of Hyperbaric Oxygen Medicine in China
Hyperbaric oxygen medicine in China began later than in Europe and the United States, but it has developed rapidly.
Before the founding of the People’s Republic of China, the Shanghai Salvage Bureau was equipped with hyperbaric oxygen chambers to prevent and treat decompression sickness in divers.
In 1954, the Naval Medical Research Institute constructed a hyperbaric chamber and became the first in the country to use hyperbaric oxygen to treat decompression sickness and hypoxia.
In the early 1960s, hyperbaric oxygen therapy began to be used to treat gas gangrene, vasculitis, cerebral edema, drowning, and other conditions.
In 1963, Premier Zhou Enlai made a special inspection visit to Shanghai to review the country’s hyperbaric oxygen medicine efforts and stated: “Diving medicine is a new and very important discipline in our country! I hope you will work hard to develop this field.”
In 1964, Professor Li Wenren established China’s first medical hyperbaric oxygen chamber at Xiehe Hospital, affiliated with Fujian Medical University, and performed cardiac surgery within the chamber. Professor Li Wenren’s team achieved significant results by performing open-heart surgery with extracorporeal circulation inside the hyperbaric oxygen chamber, combined with hypothermia, to repair atrial and ventricular septal defects, among other procedures, which garnered considerable attention from the domestic medical community.
In the 1970s, China began applying hyperbaric oxygen therapy to treat hypoxic-ischemic encephalopathy in newborns and infants, achieving favorable outcomes. Extensive case observations confirmed that the toxic side effects of hyperbaric oxygen on the eyes of infants and young children were far less severe than previously described. Recent studies have found that strictly controlled, standard-dose hyperbaric oxygen does not cause significant eye damage; conversely, prolonged exposure to high-concentration ambient oxygen can lead to severe eye damage.
In 1984, China manufactured its first hyperbaric chamber specifically designed for infants and young children and put it into clinical use; since then, the application of hyperbaric oxygen therapy in the treatment of pediatric diseases has developed rapidly.
In 1992, the Hyperbaric Medicine Branch of the Chinese Medical Association was formally established in Lanzhou, with Professor Li Wenren serving as the first Chair.
In 1993, the 11th International Congress of Hyperbaric Medicine was held in Fuzhou.
After 1995, China placed particular emphasis on strengthening safety management in the clinical application of hyperbaric oxygen therapy. With approval from the Medical Administration Department of the Ministry of Health, national hyperbaric oxygen certification training centers were established in Changsha and Shanghai on January 20, 1995. At the same time, national standards and safety operating procedures for medical hyperbaric chambers were formulated, standardizing the production and management of medical hyperbaric chambers, thereby putting China’s hyperbaric oxygen therapy on a path of healthy development.
In 1996, the Hyperbaric Medicine Branch of the Chinese Medical Association formulated the “Regulations on the Management and Application of Medical Hyperbaric Chambers,” which outlined the indications and contraindications for hyperbaric oxygen therapy. That same year, Hunan Medical University included hyperbaric medicine as an elective course in its undergraduate curriculum and began training master’s degree candidates in hyperbaric medicine.
In 2008, the 16th International Congress of Hyperbaric Medicine was held in Beijing.
In 2008, the First Affiliated Hospital of China Medical University purchased a new hyperbaric chamber for its Hyperbaric Medicine Department, equipped with medical devices such as monitors and ventilators. This became the nation’s first ICU hyperbaric chamber, providing a reliable treatment platform for the resuscitation of critically ill patients within the hyperbaric chamber.
In 2013, the National Health and Family Planning Commission officially released the standard titled “Technical Specifications for the Clinical Application of Hyperbaric Oxygen Therapy,” which took effect on November 1, 2013, under the implementation code WS/T 422-2013.
Since the beginning of the 21st century, hyperbaric oxygen therapy has developed rapidly in China, becoming widespread in county-level hospitals, and some township hospitals below the county level have also begun offering hyperbaric oxygen therapy.
In 2018, the Hyperbaric Medicine Branch of the Chinese Medical Association revised the “Specifications for the Safety Management and Application of Medical Hyperbaric Chambers” and updated the indications and contraindications for hyperbaric oxygen therapy.
Currently, hyperbaric oxygen therapy is used to treat more than 100 clinical conditions in China. For some conditions, hyperbaric oxygen therapy has become a standard treatment, such as carbon monoxide poisoning, anaerobic bacterial infections, air embolism, decompression sickness, anesthetic complications, hypoxic encephalopathy, cerebral infarction, encephalitis, sudden deafness, traumatic brain injury, replantation of amputated fingers, skin grafting, scalds, burns, chronic ulcers, poisoning, and various types of altered consciousness where active intracranial hemorrhage has been ruled out.
3. The Future of Hyperbaric Oxygen Medicine
Over the past two decades, as research in various fields has deepened and multidisciplinary collaboration has expanded, the methods for diagnosing and treating diseases in clinical medicine have undergone revolutionary changes. Building on the ongoing standardization of the scope of diseases treated and specific treatment protocols, hyperbaric oxygen medicine—both now and in the future—will also leverage scientific and technological innovations to pioneer new models of hyperbaric oxygen medicine. Hyperbaric oxygen medicine will continue to break new ground in areas ranging from equipment upgrades to therapeutic innovations, from the deepening of fundamental theories to personalized clinical treatments, and from the widespread adoption of clinical practices to teaching and research.
3.1 Advanced Development of Hyperbaric Oxygen Chamber Facilities and Equipment
With the continuous development and innovation of medical science and technology in China, hyperbaric oxygen chamber facilities and equipment are also being constantly updated. The emergence and widespread adoption of circular chambers, circular flat-bottomed chambers, and square chambers have enhanced patient comfort during treatment. In the future, the advent of mobile hyperbaric oxygen chambers will facilitate the treatment and emergency rescue of patients during large-scale public health emergencies. Regions will flexibly adjust the distribution of hyperbaric oxygen chambers and hyperbaric treatment protocols in wards based on demand, and establish provincial, national, and even global hyperbaric medicine alliances. At that time, mobile hyperbaric oxygen chambers will benefit more critically ill patients and extend coverage to more remote and underdeveloped areas. Similarly, the components of hyperbaric oxygen chambers—such as chamber doors, pressurization systems, respiratory devices, communication systems, fire safety equipment, and computer systems—are becoming increasingly sophisticated in design, cutting-edge in performance, and comprehensive in functionality. Chamber doors feature a sliding mechanism that is easy to operate and locks securely; pressurization systems are quiet, provide ample gas supply, and are of high quality; respiratory systems deliver fresh oxygen, ensure a calm breathing experience, and facilitate smooth exhalation; the communication system offers clear, visible audio and video coverage throughout the entire process, from all angles, with easy storage and playback; the fire suppression system ensures safety through automatic detection, prediction, and preemptive response; and the computer system operates smoothly, with seamless workflows and intuitive human-machine interaction.
At the same time, the range of in-chamber equipment has gradually diversified to fully meet the needs of clinical hyperbaric oxygen therapy for patients. In addition to the equipment already widely used in chambers—such as oxygen masks and connecting tubing, negative-pressure suction devices, cardiac and cerebral electrocardiogram monitoring, in-chamber ventilators, and transcutaneous oxygen saturation monitors—in-chamber cardiopulmonary resuscitation devices, endotracheal intubation equipment, in-chamber intravenous infusion sets, in-chamber rehabilitation exercise equipment, and spinal traction devices, as well as equipment for assessing patients’ conditions, such as electroencephalographs (EEGs), blood gas and hemorheology analyzers, intracranial pressure and cerebrospinal fluid partial pressure of oxygen monitors, fundoscopes, blood glucose meters, and dynamometers for measuring muscle spasms.
To meet the needs of scientific research, the field of animal experimentation hyperbaric chambers is no longer limited to general animal studies; experimental hyperbaric chambers for cell culture, genomics, proteomics, and other scientific research are increasingly being used in hyperbaric oxygen research.
3.2 Personalized Hyperbaric Oxygen Therapy
Personalized hyperbaric oxygen therapy is a key direction in the current and future development of hyperbaric medicine. It began in the 1980s, when Dr. Richard Neubauer first used single-photon emission computed tomography (SPECT) to assess the response of individual stroke patients to hyperbaric oxygen therapy. In the current post-genomic era, genes can be viewed as biomarkers of response to hyperbaric oxygen therapy and predictors of oxygen toxicity, which will help determine the appropriateness of hyperbaric oxygen therapy for each patient, as well as the optimal treatment pressure and duration.
To keep pace with the trend toward personalized hyperbaric oxygen therapy, further molecular research related to hyperbaric oxygen is needed, such as: basic research on the molecular mechanisms underlying the effects of hyperbaric oxygen; genomic studies on the response to hyperbaric oxygen therapy to obtain genomic information associated with a response or lack of response to hyperbaric oxygen; and pharmacogenomics and pharmacogenetics studies on oxygen toxicity associated with hyperbaric oxygen therapy.
3.3 The Role of Hyperbaric Oxygen Therapy in Future Multidisciplinary Healthcare Systems
Clinical medicine is evolving into a multidisciplinary field. An increasing number of diseases require the discussion and integration of multiple treatment options to develop comprehensive treatment plans that are most beneficial to patients. Consequently, hyperbaric oxygen therapy is likely to be combined with an increasing number of new therapeutic modalities. For example, regenerative technologies can be integrated with hyperbaric oxygen therapy for fracture repair and wound healing. Furthermore, as the medical concept of “tertiary prevention” (etiological prevention, preclinical prevention, and clinical prevention to promote rehabilitation) gains deeper traction, the role of hyperbaric oxygen therapy in tertiary prevention for certain diseases—particularly chronic conditions—will become increasingly prominent. For example, hyperbaric oxygen therapy can prevent the onset of ischemic cerebrovascular disease at its root cause in patients with stenosis of the major cerebral blood vessels; for patients with unstable carotid plaques, it can prevent or delay the occurrence of cerebral infarction; and for patients in the recovery phase of stroke, it can reduce disability rates, promote neurological recovery, and accelerate the rehabilitation process.
3.4 In-Depth Development of Hyperbaric Oxygen Medicine
Over the coming decades, hyperbaric oxygen medicine itself will also undergo significant development. First, as research into the molecular theory of hyperbaric oxygen deepens, clinical trials flourish, and evidence-based medical data continues to accumulate, the mechanisms underlying hyperbaric oxygen therapy will become clearer, the scope of treatable conditions will expand, and treatment options will become more diverse; Second, continuous innovation in hyperbaric chamber equipment and the ongoing development of instruments usable within the chambers will enable patients to undergo a wider range of higher-quality diagnostic tests and treatments inside the chambers, thereby integrating hyperbaric medicine more closely into clinical practice; Finally, the discipline of hyperbaric medicine itself will gradually evolve from a peripheral clinical discipline focused primarily on disease treatment into a comprehensive field encompassing research on the etiology, diagnosis, treatment, and prognosis of specialized conditions. As the discipline matures and develops, treatment facilities will no longer be limited to treatment centers but will instead feature a comprehensive system of outpatient clinics, inpatient wards, and treatment centers tailored to the specific diseases and patients within this specialty. To ensure the sustainable development of the discipline, hyperbaric medicine will place greater emphasis on research and education, forming a complete disciplinary system that balances clinical practice, research, and teaching.
3.5 Future Needs of Hyperbaric Medicine
To ensure that hyperbaric medicine keeps pace with developments in other medical fields, the following measures are recommended: ① Continuously improve hyperbaric chamber equipment and facilities, and introduce new in-chamber diagnostic and therapeutic technologies based on specific medical needs; ② Deepen research; hyperbaric physicians need to become familiar with new biotechnologies and their potential applications in combination with hyperbaric oxygen therapy; ③ Expand the scope of clinical applications by combining hyperbaric oxygen therapy with other treatment methods; ④ Optimize treatment protocols, strengthen the management of treatment timelines, and adopt personalized treatment plans whenever possible; ⑤ Enhance the training and management of practitioners to improve the quality and safety of hyperbaric oxygen therapy.

